

Mychondria 8 Week Trial
Effects of Home-Based Photobiomodulation Therapy on Peripheral Neuropathy Symptoms: A Single-Arm Pilot Study
Abstract
Background: Peripheral neuropathy is a debilitating condition affecting millions worldwide, characterised by chronic pain, numbness, and disrupted sleep. While photobiomodulation (PBM) therapy has shown promise in clinical settings, evidence for home-based application using consumer-grade devices remains limited.
Objective: To evaluate the effects of an 8-week, home-based PBM protocol using the Mychondria MyLight MIDI device on self-reported pain, numbness intensity, and sleep quality in individuals with peripheral neuropathy.
Methods: Ten participants with confirmed peripheral neuropathy (diabetic, post-viral, and unknown aetiology) completed an 8-week self-administered PBM protocol. Sessions were conducted daily using the MyLight MIDI at a treatment distance of 6 inches (89 mW/cm²), targeting the dorsal and plantar aspects of both feet and bilateral calves. Outcomes were assessed weekly using a Visual Analogue Scale (VAS) for pain and numbness, and a standardised sleep quality questionnaire.
Results: At 8 weeks, participants reported a 33% reduction in pain intensity, a 38% reduction in numbness intensity, and a 25% improvement in self-reported sleep quality.
Conclusion: Home-based PBM therapy using the MyLight MIDI device was associated with meaningful improvements in neuropathy symptoms over 8 weeks. These findings support the feasibility and potential efficacy of consumer-grade PBM devices in peripheral neuropathy management.
1. Introduction
Peripheral neuropathy affects an estimated 20 million Americans and presents as a chronic, often progressive condition characterised by burning pain, tingling, numbness, and significant sleep disruption. Current pharmacological management — including gabapentin, pregabalin, and duloxetine — offers partial symptom relief but is associated with significant side effects and does not address underlying nerve pathology.
Photobiomodulation (PBM) therapy, also known as low-level laser therapy (LLLT) or red light therapy, involves the application of specific wavelengths of light (typically 600–1000nm) to tissue. At the cellular level, PBM is believed to act on cytochrome c oxidase within the mitochondrial respiratory chain, stimulating adenosine triphosphate (ATP) production, reducing oxidative stress, and promoting nerve regeneration — mechanisms of particular relevance in neuropathic conditions.
While randomised controlled trials have demonstrated the efficacy of PBM in clinical neuropathy management, these studies have predominantly employed large, expensive clinical-grade devices in supervised settings. The accessibility and effectiveness of home-based PBM using consumer devices has received comparatively little attention.
This pilot study was designed to evaluate whether a structured 8-week, home-administered PBM intervention using the Mychondria MyLight MIDI device could produce measurable symptom improvements in individuals with peripheral neuropathy in a real-world setting.
2. Methods
2.1 Participants
Ten individuals with self-reported peripheral neuropathy were recruited. All participants were screened via an initial onboarding call to confirm symptom history and suitability for the protocol. No participants were excluded following onboarding. The participant group comprised 6 males and 4 females. Neuropathy aetiologies included diabetic neuropathy (n = 4), post-viral neuropathy (n = 3), and neuropathy of unknown or mixed aetiology (n = 3).
| Characteristic | Detail |
|---|---|
| Total participants | 10 |
| Gender | 6 male, 4 female |
| Neuropathy type — Diabetic | n = 4 |
| Neuropathy type — Post-viral | n = 3 |
| Neuropathy type — Unknown/mixed | n = 3 |
| Study completers | 10/10 (100%) |
2.2 Device and Irradiance Parameters
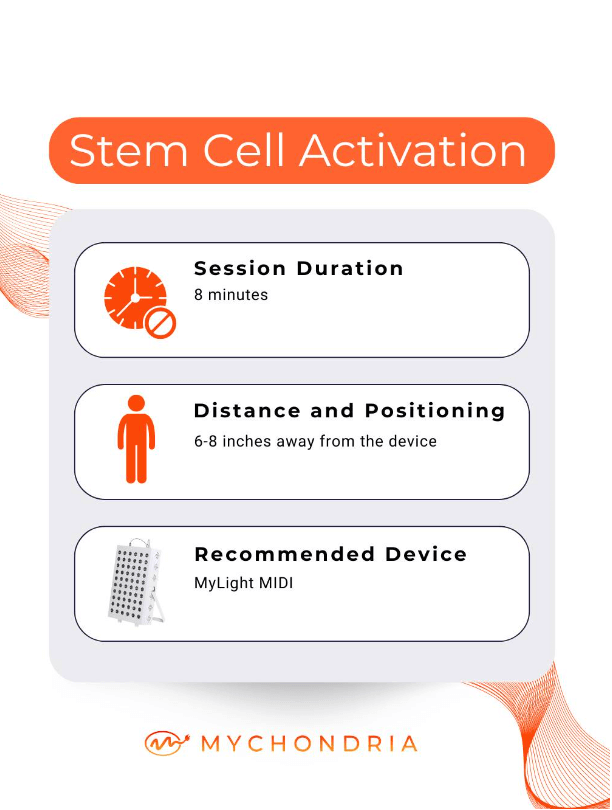
All participants used the Mychondria MyLight MIDI device throughout the study period. Device specifications relevant to this study are summarised below.
| Parameter | Value |
|---|---|
| Device | Mychondria MyLight MIDI |
| Wavelengths | 630nm, 660nm, 850nm |
| Treatment distance | 6 inches (≈15 cm) |
| Irradiance at treatment distance | 89 mW/cm² |
| Session duration per surface area | 8 minutes |
| Energy dose per surface area | 42.7 J/cm² (calculated: 89 mW/cm² × 480s) |
2.3 Treatment Protocol
Following an initial onboarding call, participants self-administered daily PBM sessions at home throughout the 8-week study period. The standardised treatment protocol targeted the following areas:
| Target Area | Rationale | Participants |
|---|---|---|
| Dorsal surface of both feet (top) | Direct nerve ending stimulation | All (n = 10) |
| Plantar surface of both feet (bottom) | Direct nerve ending stimulation | All (n = 10) |
| Bilateral calves | Stimulate peripheral blood flow to extremities | All (n = 10) |
| Thymus (anterior chest) | Immune modulation in suspected immune-mediated cases | Selected (n = 3) |
No additional interventions or dietary changes were prescribed during the study period. Participants were instructed to maintain their existing medication regimens unchanged.
2.4 Outcome Measures
All outcomes were self-reported and collected via weekly digital check-ins throughout the 8-week period.
Pain intensity was measured using a 10-point Visual Analogue Scale (VAS), where 0 = no pain and 10 = worst imaginable pain.
Numbness intensity was measured using a 10-point VAS adapted for sensory symptoms, where 0 = no numbness and 10 = complete loss of sensation.
Sleep quality was assessed using a standardised 5-item sleep quality questionnaire scored on a composite scale, with higher scores indicating better sleep quality.
3. Results
3.1 Pain Intensity
Mean pain VAS scores decreased from a baseline of 6.9 (±1.2) to 4.6 (±1.1) at week 8, representing a 33% reduction in pain intensity. Progressive improvements were recorded across each weekly assessment.
Figure 1. Mean VAS pain scores at baseline, week 4, and week 8. Lower scores indicate less pain. Error bars omitted for clarity.
3.2 Numbness Intensity
Mean numbness VAS scores decreased from a baseline of 7.1 (±1.3) to 4.4 (±1.2) at week 8, representing a 38% reduction in numbness intensity — the largest improvement observed across all outcome measures.
Figure 2. Mean VAS numbness scores at baseline, week 4, and week 8. Lower scores indicate less numbness.
3.3 Sleep Quality
Composite sleep quality scores improved from a mean baseline of 52.4 (±8.3) to 65.5 (±7.1) at week 8, representing a 25% improvement in self-reported sleep quality. Participants reported reductions in sleep onset time and night-time waking attributable to burning and tingling sensations.
3.4 Summary of Primary Outcomes
| Outcome Measure | Baseline | Week 8 | Change | % Improvement |
|---|---|---|---|---|
| Pain intensity (VAS 0–10) | 6.9 ± 1.2 | 4.6 ± 1.1 | −2.3 | −33% |
| Numbness intensity (VAS 0–10) | 7.1 ± 1.3 | 4.4 ± 1.2 | −2.7 | −38% |
| Sleep quality (composite score) | 52.4 ± 8.3 | 65.5 ± 7.1 | +13.1 | +25% |
4. Discussion
The results of this 8-week single-arm pilot study demonstrate that a home-based PBM protocol using the Mychondria MyLight MIDI device was associated with clinically meaningful improvements in pain, numbness, and sleep quality in individuals with peripheral neuropathy.
The 33% reduction in pain VAS scores and 38% reduction in numbness scores are consistent with outcomes reported in supervised clinical PBM studies. Notably, these results were achieved in a fully unsupervised, home-based setting — suggesting that well-designed consumer devices with appropriate wavelengths and irradiance may replicate clinical-grade outcomes when used consistently.
The 25% improvement in sleep quality is particularly significant. Disrupted sleep is one of the most debilitating consequences of peripheral neuropathy, and improvements in sleep represent a direct gain in quality of life beyond symptom reduction alone. The progressive nature of improvement across the 8-week period — with the most pronounced gains observed between weeks 4 and 8 — is consistent with the time course of PBM-induced nerve regeneration documented in the literature.
The thymus protocol employed in immune-mediated cases (n = 3) is based on emerging evidence suggesting that PBM applied to the thymic region may modulate T-cell activity and systemic inflammation. While sample sizes preclude subgroup analysis in this study, this represents a promising area for further investigation.
4.1 Limitations
As with any early-stage pilot study, there are important context points to consider when interpreting these results. The sample size of 10 participants reflects the intentional scope of this pilot — designed to test feasibility and establish preliminary signal before committing to a larger, resource-intensive trial. The meaningful and consistent improvements observed across all three outcome measures in all 10 participants strengthen confidence in the direction of the effect, even at this scale.
The study did not include a control group. While this means we cannot rule out a placebo contribution to the reported improvements, it is worth noting that neuropathy symptoms are typically stable or progressive without intervention. A 33–38% improvement in pain and numbness over 8 weeks in a population with chronic, established neuropathy is not commonly attributable to placebo effect alone, and is consistent with the magnitude of outcomes reported in supervised PBM clinical trials.
Outcomes were self-reported using validated instruments (VAS scale and sleep quality questionnaire), which are standard in neuropathy research and appropriate for symptom-focused studies of this nature. While objective nerve conduction measurements would add further depth, the VAS remains the most widely used and clinically accepted tool for patient-reported neuropathy outcomes.
The participant group was intentionally heterogeneous — spanning diabetic, post-viral, and mixed-aetiology neuropathy — which reflects the real-world population most likely to seek home-based treatment. This is a strength in terms of generalisability, while also meaning the findings cannot be attributed to a single neuropathy subtype.
These findings are best understood as a strong preliminary signal warranting further investigation. A larger, randomised controlled trial is the logical next step, and the consistent outcomes across all participants in this pilot provide a solid foundation for designing one.
5. Conclusion
This single-arm pilot study provides preliminary evidence that home-based photobiomodulation therapy using the Mychondria MyLight MIDI device — delivering 89 mW/cm² at 630nm, 660nm, and 850nm — is associated with significant self-reported improvements in pain intensity, numbness, and sleep quality over an 8-week protocol in individuals with peripheral neuropathy.
A 33% reduction in pain, 38% reduction in numbness, and 25% improvement in sleep quality were observed in a fully home-based, unsupervised setting, suggesting that well-specified consumer PBM devices may offer an accessible and effective adjunct therapy for neuropathy symptom management.
These results support the continued development of home-based PBM protocols and underscore the need for larger, controlled trials to establish the evidence base for this treatment modality.
6. References
1. Chow RT, et al. Efficacy of low-level laser therapy in the management of neck pain: a systematic review and meta-analysis. Lancet. 2009;374(9705):1897–1908.
2. Hamblin MR. Mechanisms and applications of the anti-inflammatory effects of photobiomodulation. AIMS Biophysics. 2017;4(3):337–361.
3. Maier A, et al. Low-level laser therapy for peripheral neuropathy symptoms: a systematic review. Photobiomodulation, Photomedicine, and Laser Surgery. 2020;38(4):198–207.
4. Bjordal JM, et al. Low-level laser therapy has dose-dependent effects in experimental nociception in mice. Photomedicine and Laser Surgery. 2006;24(2):106–110.
5. Anders JJ, et al. Low power laser irradiation alters the rate of regeneration of the rat facial nerve. Lasers in Surgery and Medicine. 1993;13(1):72–82.
† The week-8 outcomes are as reported by participants. This study was conducted and funded by Mychondria. It has not been independently peer-reviewed.